As a support network for neurodivergent police officers and staff, one of our most frequently-asked questions concerns reasonable adjustments. A reasonable adjustment is defined as a change in the workplace to remove or reduce the effect of an employee or job applicant’s disability, when carrying out or applying for a job. Disabled employees and applicants, including* those with neurodivergent conditions such as autism and dyslexia, are entitled to reasonable adjustments under the Equality Act to help them overcome the limitations of their disability or condition at work or in seeking employment.
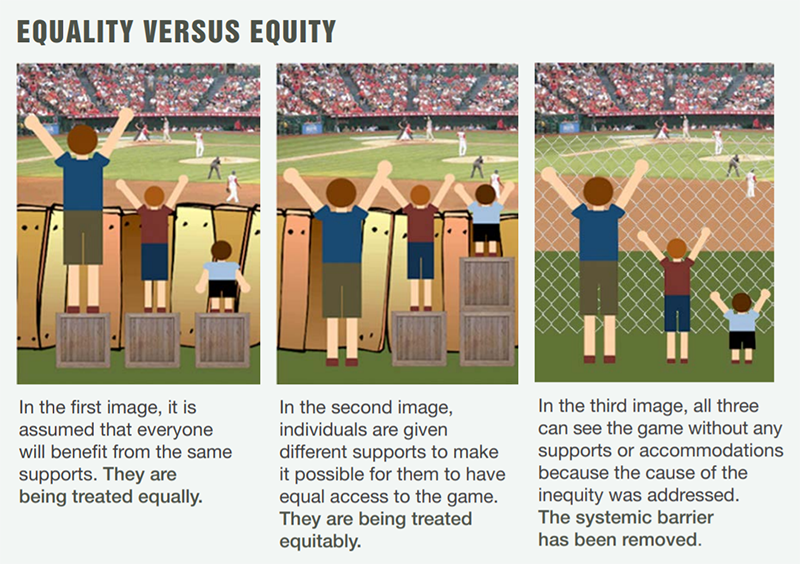
An important concept in the reasonable adjustment process is that it is sometimes necessary to treat people differently in order to provide everyone with an equal opportunity to succeed. This is best illustrated by the following graphic, created by the Canadian City for All Women Initiative:
The first image shows what can happen when everyone is treated equally – some people will lose out due to the effect of their disability or other protected characteristic. The second image shows equity, or fairness, and how this differs from equality – by giving some people additional support, everyone has an equal chance of success.
Reasonable adjustments in selection and promotion processes are sometimes misunderstood as ‘special treatment’ that gives some people an unfair advantage (and therefore disadvantages others). It’s important to understand that adjustments are there to ensure that disabled and neurodivergent applicants have the same chance of success as everyone else – the second image in the graphic. A typical example is wording the interview questions for an autistic candidate to remove any ambiguity, and allowing the candidate to have each question in writing to refer to when they provide their answer. Research by the University of Bath has shown that autistic interviewees can over-analyse or misinterpret questions and struggle to mentally organise their evidence to fit what is being asked – adjusting the style of questions, providing thinking time and written prompts allows the candidate to overcome these difficulties and present themselves as well as other applicants. (Candidates with dyslexia and other neurodivergent conditions may also benefit from these adjustments.)
Continuing the example of workplace interviews, some employers have gone a step further by providing all candidates with neurodivergent-friendly questions, preparation time and written prompts. This is an example of the third image in the graphic – removing the systemic barrier so that no one is disadvantaged or needs to ask for adjustments. With a little thought and effort, this approach can be applied to any workplace environment, process or culture – and as with the interview example, it has the potential to benefit everyone, disabled or not. ∎
*Neurodivergent conditions may meet the criteria of a disability – assessed on an individual basis
In this personal account, Ministry of Defence Police Sergeant Dan Harris reflects on his ADHD diagnosis and how his understanding of the condition allowed him to recognise his strengths and achievements
I first started writing this blog based around my experience of ADHD in January 2021. The original draft contained gems of information encased in multiple layers of drivel that would likely reduce the reader to abandonment after a few lines. I felt the article needed to relay my journey in terms of pre- and post-diagnosis and how it impacted on my life during both phases due to the traits. On reading it through, it felt like a monotonous trudge along a barren motorway.
I once spoke to a fellow police service ADHD-er – what struck me about this individual was their extraordinary positivity regarding their condition. In my mind, I remember thinking that we were looking at the condition from two completely different perspectives; and for the briefest of moments, through this dialogue I was able to experience how they completely accepted and embraced each aspect of ADHD lovingly and with no judgement. I momentarily wore their perspective like an item of clothing, hoping it would fit. This was a garment they had spent significant time lovingly weaving, but regrettably I just couldn’t get it to stay in place; it felt wrong and it didn’t conform. I concluded that my colleague’s life experiences had been significantly kinder than mine.
My personal journey into ADHD did not commence until 2018. I am now 45 years of age so its fair to say I have spent a significant portion of my life not knowing I had this condition. Sadly, this is not unusual as ADHD is only really observed (usually by others) when it explodes in what can only be described as uncontrollable behaviour, which more commonly manifests in young male children. It’s a sorry situation when a condition is only treated or noticed when it becomes intolerable, but sadly this lack of understanding is not just confined to ADHD – it’s endemic in most neurodivergent conditions.
Media coverage has most likely perpetuated the stereotyping that exists around ADHD, and if this is the fire then some professionals who are perhaps ill-informed and really ought to know better must surely be the fuel. A significant problem here is that most stereotyped ADHD behaviour appears typical in young males, and since some can mask this behaviour as they grow older, it perpetuates the damaging perception that ADHD is a childhood condition. There are also other negative connotations: many females are either are not as aggressive with the condition – and thus more malleable – or they struggle with the attention deficit element which is again less obvious to spot. But of even more significance is not all males with the condition can be expected to conform to the stereotypical norm either, and their chances of being diagnosed are even more significantly reduced, as is evidenced by both my son and I.
My own diagnosis came about after my son was diagnosed as there were similarities between us. However, my son excelled during his initial schooling and then seemingly fell into a precipice when he had to take responsibility for his own learning on conclusion of secondary education. Sadly, by comparison I struggled with the early part of schooling and whilst I was respectful and well-behaved, I never really achieved much in the initial schooling years. During my personal exploration pre-diagnosis there were elements of ADHD that seemed to resonate with me and an online screening test via the informative Additude website seemed to strongly suggest I might have the condition. At around this time I had informed my line manager of my desire to seek diagnosis and he responded by stating “Why do you want to go and get yourself a label?” I clearly remember the time of day, the room we were stood in and the wave of anger that I managed to stifle as I explained why this was so important to me.
Whilst I was finishing off my first draft of this blog, the above incident was one of many I can recount since diagnosis, and I reflected on childhood more than I have ever done before. I could seldom remember a positive word written by teachers in my school reports, and perhaps even sadder is that my parents cared even less because they had zero expectations of me and had effectively written me off at a young age through comparisons with my three older siblings. Until I started writing this piece, I held great resentment towards them post-diagnosis. However, I had an epiphany that now deeply resonates: I had become everything they believed me to be, and this became deeply ingrained. Comments on my old school reports may strike a chord with some of you; in my day I theorised that teachers must have held rubber stamps to be wielded on those pupils who were somewhat beyond their teaching abilities. I knew they used to talk in the staff room, and I believed they must have shared the same labels and used them every year on my reports. My stamps were: “needs to pay attention”, “easily distracted by others”, “has proven on occasions that he is able, but is simply not trying hard enough”, “nice lad tries hard”, and so on. One teacher once got so frustrated when I expressed concerns over an inability to grasp his teaching that he informed me I would amount to nothing, becoming a person subjected to the ‘mushroom theory’. To my delight he then embellished this further, informing me that I would be locked in a dark room my entire life and fed on excrement (he of course used the somewhat more common word!) This was the first and only time that I learned something in one of his lessons.
I cannot thank the NPAA enough for allowing me to write this blog, as it led to something quite profound happening. When reflecting on my past I began recounting all the self-perceived negative traits of my condition, and then linked them to moments where I had failed in one way or another. I had forgotten about school reports, lack of belief from parents and most (but not all) teachers. I thought about profound moments of failure and directly linked them to my condition – I had done this since diagnosis with more recent failures, so going back further wasn’t too difficult. The defining moment however came in an extremely rare moment of stillness: in my mind, I pondered on why I needed to perceive my condition so negatively. At first, I thought it could be down to my turbulent experience since diagnosis and my battle to have my condition accepted. But in the end, the real reason needed that moment of stillness in order to cut through negative self-perception.
After diagnosis I searched for signs of all the negative traits synonymous with ADHD, and with every passing day I discovered something new, leaving little point in looking too far back in my life. The condition is held in such poor esteem, and some will question its existence even in the face of overwhelming evidence. If you are new to ADHD, can you immediately identify any positive traits of the condition as you read this blog? The poor perceptions and stereotypical views were the perspective that I was judging myself from, and it was from this basis that I was searching for evidence to justify my diagnosis to others. The problem being the more I did it, the more people normalised some of my traits which I made me feel like they were being dismissive and simply added further frustration.
It’s impossible to ignore the negative elements of my condition, especially in challenging environments where there is very little support, but I now know I can now choose how I allow these moments to affect me. I can continue championing the condition whilst educating others, and I can now stop searching for those negative traits and celebrate the positive ones. During my attempts to justify the existence of my condition, others were keen to highlight minor successes as if they were some huge significant achievement, but the reality was these were relatively ordinary in comparison to my neurotypical peers. Colleagues with similar intelligence had easily negotiated these hurdles and beyond, and many had left me behind in my 22 year career including student officers I had trained. My perception was that these minor achievements were being highlighted to qualify my colleagues’ rationale for not needing to support me. Far worse though were the feelings that they were effectively suggesting I had achieved so much for a person with ADHD.
My perception of self has now changed thanks to this blog, and I no longer view it from that old perspective. Writing this piece caused a period of reflection where I suddenly diverted from my old destination in favour of a much shorter and more interesting route. I now know that very few of my neurotypical peers would have been able to overcome the mental barriers I overcame over the years, even if my achievements in doing so were mundane compared to what they achieved. Few will have picked themselves up from continual rejection and displayed an almost superhuman forms of resilience. Better still, I also realised I had a unique set of gifts afforded to me that were gathering dust due to my former misdirected focus. I am learning to weave a garment from my own unique brand of ADHD which fits me perfectly, and if a person can’t accept who I am that says more about them than me.
I will now present my former perspective of my ADHD and follow with a more positive perspective – but first, a common quote which resonates with me: “If you judge a fish by its ability to climb a tree, it will live its whole life believing it is stupid”. This is credited to Albert Einstein, whom many have suspected was ADHD.
There are times in my life where I have been left frustrated by my carelessness and this has resulted in failing in some aspirations when competing with other people. ADHD has gifted me with high levels of resilience and taught me how to bounce back from rejection and failure.
I can be terribly messy and leave things lying around. My ADHD creates a phenomenon where items cease to exist until I am reminded of them, and then searching for them can be frustrating and take time. As a coping mechanism I place things in line of site where they are never forgotten – I also habitually place them in the same location, although this can seem messy to others. (See Einstein’s desk for example.) Whilst this niggles my neurotypical colleagues, this simple process highlights my highly adaptable abilities as my differently wired brain finds ways to adapt to its neurotypical foreign environment. I am the fish out of water.
My disorganisation can lead to tasks being missed. I have a superpower of hyperfocus which provides me with boundless energy to keep going until a task is complete and within the deadline. I do sometimes miss deadlines, and I occasionally miss non-critical deadlines in an unsupported environment. However, when there is an urgent task you can rely on my extreme energy levels and hyperfocus to kick and see the task through to completion with seconds to spare.
I can’t prioritise and can only manage one small task at a time. I now realise this was a mis-sold perception that I invested far too much time and belief in. I can in fact multi-task – see above for those critical deadlines! ADHD folk benefit from breaking down tasks into short sprints affording each with a ‘win’ at the end. I had previously been trying to apply neurotypical techniques, and it was this approach that created disastrous results.
I hardly sleep compared to others. Some nights I just can’t stop my brain from its constant internal dialogue, and no matter how hard I try I just don’t seem to get a quality night’s sleep. During these times when others are deep in the land of nod, my brain seeks solutions to problems and it is at these times I have worked through some major issues. Whilst I sleep less, I actually feel no worse for it – in fact on the rare occasions when I am able to sleep, I find my brain is less alert.
I am easily distracted and miss things all the time. How can I possibly take a positive from that? Well it turns out that the attention deficit element of my condition is not a lack of attention, but is actually related to too much attention. ADHD folk lack the chemical dopamine which is the feel-good chemical that motivates neurotypical people to complete tasks. My brain is constantly scanning for things to stimulate the brain. This ability was also essential in prehistoric times as my people were able to constantly scan for dangers. ADHD folk were the pathfinders back in the day. My peripheral vision is constantly scanning, so it comes into its own when driving.
Other positives of my own brand which I know many others share are an unbounding energy and enthusiasm, extreme levels of resilience, and an ability to think outside the box. In fact rather than thinking outside the box I just remove the boxes completely, which can be overwhelming to some of my neurotypical colleagues!
Moving forward, I will learn ways to use my gifts to my advantage: I will recognise that the external environment is structured to cater for the majority and that by making subtle adjustments I can adapt to most environments. For those where I can’t and where there is no support enabling me to thrive, I simply need to remove myself from that location and find a place where my skills will be valued and embraced. I am currently studying a master’s degree in human resource management – I had previously attempted study pre-diagnosis and suffered a spectacular crash, but this time I have appropriate support to help me overcome my disadvantages. If there is one thing I have learnt in the first twelve months its that the human resource is a valuable commodity. When we consider policing, it can be considered the main cog in the machine, and our success depends on it. Failure to maximise the potential of everyone who is a component of that machine could ultimately result in inefficiency, but worse in my eyes is that it overlooks the opportunity to achieve maximum performance and to create a happy and inclusive working environment.
If you are embarking on the same journey of discovery for ADHD or any other neurodivergent condition, my advice is this: don’t be harsh on yourself. Stop viewing the world from a neurotypical vantage point that sees your traits as negatives, and understand that you are different and special. You have unique gifts, and to steal a quote from a colleague, each of us is simply a different kind of clever. So – forget your weaknesses and seek out your strengths. ∎
by James Bird Detective Sergeant West Midlands Police
As part of National Inclusion Week, I wanted to try to write an article on dyslexia in the simplest of terms – its advantages and disadvantages and to share my experiences to provide an insight into how being ‘diagnosed’ later in life has helped me understand why I am who I am. This is in the hope that it will encourage some who read this, and who can relate to the indicators, to get an assessment.
Please try and think about your own experiences whilst reading this and see if anything that I have written rings true personally for you, whatever role or rank you are. Think about your time in school, growing up, your time at work, how you lead and how you think and solve problems. Do you like to design things, build things from scratch? Do you think in images and pictures in your mind? Are you particularly good at coming up with unique solutions to problems, hypotheses to investigations that seem obscure but turn out to be the correct solution, or manipulating information always looking at the bigger picture? Did you or your parents struggle at school with reading or writing, but had an ability to problem solve and lead when others could not? Many dyslexics have had varied careers and roles, sometimes unexplainably related to each other, in their own ways. Are you overly empathetic? These are some of the things to consider whilst reading this article.
Dyslexia is a neurodivergent learning difference (not difficulty) that affects approximately 10% of the population – however it is known that certain professions attract a higher percentage due to their very nature, such as graphic designers, architects and surgeons to name a few. Policing is identified as one of those such professions and potentially putting the percentage up to as high as 40%. The skills of individuals with dyslexia are increasingly becoming more sought-after with many police forces actively recruiting and advertising for dyslexic officers. Dyslexia is sometimes classed as a disability, depending on the individual.
Dyslexics are often creative due to being able to come up with different ways of solving problems and making decisions – they are often troubleshooters, lateral thinkers and able to give differing solutions on different subjects. They are persistent, determined and resourceful with a desire to succeed. Dyslexic brains do not function differently because they are defective but because they are organised to display different strengths at the cost of relevant weaknesses in fine processing.
I must make a point that I am by no means an expert on this subject and am happy to be corrected or challenged on certain points. I can only talk from experience and what I have read but there are far more knowledgeable people in our organisation who could give you a better context to the subject. I am not an academic or scientifically trained and most of the facts I have quoted come collectively from a number of different sources that I have read as part of my own personal understanding and journey with dyslexia. Interestingly, collating information from different sources and presenting it together as a whole to make sense of a problem, is in itself a dyslexic strength. I have included links to the resources I used to write this below, for further information and encourage you to go to the Occupational Health portal for more information on arranging an assessment.
So with all this information I have included, I would like to start off with sharing my own dyslexia experience and how being assessed has helped me, which I hope some can relate to:
For some context: I left school with a couple of CSEs, having been a slightly above average achiever. My favourite subjects were history and geography, with it being noted how I showed a particular affinity to reading maps and remembering them topographically. As the class joker, I was unable to concentrate on things for very long and struggled with learning, but with an ability to distract everyone else in the class!
Having left school, I wanted to join the WMP Police Cadets but my policing career aspirations ended as my eyesight was not good enough. (Thankfully laser eye surgery became a thing in the early 2000s). I had a number of jobs, including building performance kit cars and then pursued a number of my own businesses. I then spent the next 15 years pursuing a career in the dance music industry. This led to me running my own DJ booking agency, and having associated offices in Birmingham, NYC, Moscow and Ibiza. Presenting and talking in front of thousands of people was and is no issue for me. Then in 2005, I decided to just give it all up and join the police.
Now, I want to draw the hereditary parallels of dyslexia I mention later, and the similarities in its indicators and life choices. My father left school unable to read and write – due to dyslexia, unknown then. He became an experienced CNC machinist, taught himself to read and write, joined the Territorial Army, and with over 20 years of leadership, became Company Sergeant Major. He was also a union convenor. He remains the chairman of the Mercian Association and Vice-Chairman of the local British Legion. My grandmothers grandfather, William Johnson joined Birmingham Police in 1881 at the age of 21, went through promotion, was commended by the Chief Constable for arresting a number of burglars and rescuing seven people from a burning building. I mention him here as he was a direct descendant of Dr Samuel Johnson, who wrote A Dictionary of the English Language and has been posthumously diagnosed with Tourette syndrome, a neurodivergent difference. (Thanks to the WMP Museum Archives for the information.)
Having joined the police and struggling horrendously with the assessment centre, especially the writing parts, I passed and I was in! I moved to Brierley Hill Response team. During this time I found it really easy to link offences to other offences, and particularly being able to interpret the definitions to the crimes and using intelligence based policing. I found speaking to people and empathising was easy and learned quickly on the job. I’m outspoken (not sure if that’s a good thing) and during this time I got into trouble for saying what I thought, and how things I believed should be managed. I remember one occasion which is quite relevant in all this, as a point in time, when I was completing a course run by, ironically the very same person who assessed me and also many others for dyslexia. I had been struggling with statements and files, having to create templates for everything so I remembered what to write. Having been unsuccessful in completing the course I remember having a discussion about why I had not passed due to my difficulty around the statement writing. Me being me, I didn’t listen – and in hindsight, I wish I had.
Over the next few years I found myself taking the written and practical parts of my Sergeants exam. This is where I started to struggle in the job. It is at this point I want to note, that if you do think you have dyslexia and you are thinking about taking the exam or moving through the promotion processes, that reasonable adjustments are available at every stage of the process, both in-force and also with the College Of Policing. That said, it still is a difficult process for those with dyslexia, even with reasonable adjustments in place as everyone is different with different indicators.
Leadership is something that I find easy, but the management side and processes I found hard. In relation to the exam, I really struggled with the written part, and it felt like for some unknown reason that I needed to study twice as hard and for longer – I just thought I was stupid, because I knew how to apply the law practically. I found it easier to use patterns to remember certain parts of legislation, pictures and rules, and attending the courses was invaluable, as I was being shown pictures to remember things.
As a leader I have always found it easy to identify different solutions and problems, to make decisions whilst seeing things from all angles, and to manipulate various pieces of intelligence and information to come up with rationales which may at times have seemed obscure
My difficulties came to a head at the written exam: I spent the first 20 minutes staring at the questions, the letters moving around and having brain fog. People fidgeting around and leaving to use the toilet was overly distracting, and what concentration I did have was repeatedly broken. Luckily I was successful because once I had got past the concentration issues, I found answering these questions easy as I was able to imagine each scenario in my head, having practiced answering questions online which were written in the same way, hence conditioning my brain to cope. I was able to apply this to the National Investigators’ Exam also.
I also struggled with the practical scenario-based exam horrendously – this again because of the same visual stress. We were given scenarios to read in a short amount of time and then you had to remember procedures and apply them within five minute periods! I just couldn’t read the text. I barely scraped through on my second attempt passing by 1%, but a pass is a pass.
Then came the promotion boards. The core competencies are a minefield at the best of times, but it was and still is, impossible for me to remember them and then extract them at short notice in a structured way. A dyslexic brain isn’t able to do this without coping mechanisms. Our Force strategies and policies contain pie charts, pictures and data which is all over the page – they are very dyslexic-unfriendly and I cannot process them.
I remember my first board, which in my head I thought I did quite well on. However I failed, and on being given my feedback I was told that I did not present my evidence in the format they wanted – I was told it sounded like I was making it up. This was partially because I could not structure what they wanted and delivered the evidence jumbled up. Luckily, I winged it on my second board not worrying about core competencies because I knew I wouldn’t be able to remember them. The briefing exercise was a nightmare though, again the first 10 minutes of preparation involved me staring at the white paper. In the board, I spoke without thinking about the competencies, as I said I have no issues talking in front of people, and just presenting the best I could which was clearly enough.
As a Detective Sergeant, I found it easier to visit a scene and see what is in front of me and come up with solutions there and then. I know what needs to be done to get the results but I don’t necessarily know myself how to do it – I rely heavily on my team. I find it hard to read crime reports or PDF documents on a screen, preferring to print things off to read. Even then, I thought my eyesight was bad because the letters were blurred and moving, but the optician told me different. I spent a very long time struggling with stress and the subsequent anger at work, but could not understand why because I couldn’t see what the trigger was, as I was able to manage my situation, team and investigations easily.
As a leader I have always found I have a skill to speak out and question people around their decisions, raise points and challenge at any rank, face to face without fear and with empathy. I always found it easy to identify different solutions and problems, to make decisions whilst seeing things from all angles, and to manipulate various pieces of intelligence and information to come up with rationales which may at times have seemed obscure. For me this was frustrating because these abilities were not always received favourably, as they were not a standard response.
It was following taking the Inspectors exam and realising how difficult it was again to study and the issues I was having reading reports, that I decided to get tested for dyslexia. I was having no issues with big picture thinking but I was struggling with the finer details of new policies and procedures, which with all the change in the Force were coming thick and fast.
The dyslexia test involves the use of various coloured overlays to assess visual stress, then an online assessment which tests various elements such as accuracy, sequencing, memory etc. I was found to be dyslexic and reasonable adjustments were suggested. It was also noted I may have indicators of dyspraxia, but at the time of writing West Midlands Police does not test for this.
My reasonable adjustments included the use of coloured screen overlays and overlays to use when reading. These have helped my visual stress no end – the letters actually stay still most of the time! It is suggested I have 25% more time to process information and that I use ClaroRead and Dragon software, which are both designed to assist by reading text and converting it to audio, which has helped. Unfortunately these are not always compatible with our IT systems. I use yellow paper and send emails with yellow background – always a good conversation starter! Even the font and the letter spacing I am writing in now helps me with my writing.
Using these mechanisms to cope with the trade-offs of dyslexia have helped no end, especially around the stress and an understanding of why I am as I am. It has helped me think about what I am doing in these contexts. I am prone to challenging and over-talking, mainly because I now understand my brain is processing information differently and I need to get the information out before I forget. I understand if I’m not looking at someone, I’m not listening to them due to distractions. I feel like I’m a lot more focussed in the things I do also, which is why I would ask anyone who has experienced the same things to consider getting tested.
The police service now has a number of assessors across the country – the help is there, you just have to take the step. Reasonable adjustments are available for all stages of the promotion process including the exams, as well as interview processes for positions within our Force, for those with dyslexia or any other disability. West Midlands Police is a Disability Confident Leader.
What is dyslexia? Facts & myths
Dyslexia is a unique learning difference that is not connected to intelligence. People with dyslexia are not slow, stupid or thick – their brains just work differently. I’m sure no one would describe Albert Einstein or Steve Jobs as thick, both were dyslexic! Those with dyslexia have it, and it lives with them. If someone is described as having mild dyslexia it means they have dyslexia, it just affects them mildly. It is a lifelong condition that can challenge somebody every day. As more is understood about dyslexia, it is easier to understand the causes and indicators. Each individual with dyslexia has unique strengths and weaknesses. Dyslexia can be hereditary and it is found that parents with dyslexia have about a 40% chance of having a child with the same condition.
Contrary to popular misconception, dyslexia is not only about literacy, although weaknesses in literacy are often the most visible sign. Dyslexia affects the way information is processed, stored and retrieved, with problems of memory, speed of processing, time perception, organisation and sequencing. It is a reflection of a different pattern of brain organisation and information processing that creates strengths as well as challenges. These are of course connected, and are best understood as trade-offs. They often show strengths in big picture processing although they may struggle with fine-detail processing, something I have identified with myself.
Another common and well known indicator is visual stress: text can appear distorted and words or letters appear to move or become blurred. White paper or backgrounds can appear too dazzling and make print hard to decipher. This is as a result of the fine detail trade-off. The use of colour overlays is a common adjustment to reduce the stress, and the majority of (but not all) negative indicators can be addressed with reasonable adjustments.
Many people with dyslexia successfully develop and implement coping strategies, which is why sometimes people live with dyslexia without it being identified. Many people are able to compensate through technology, reliance on others and an array of self-help mechanisms, the operation of which require sustained effort and energy. Unfortunately these strategies are prone to break down under stressful conditions which impinge on areas of weakness. People with dyslexia are particularly susceptible to stress, compared with the ordinary population, with the result that their impairments become even more pronounced.
Other related learning differences include:
Dyspraxia which is a difficulty with co-ordination and the organisation of movement, anxiety in unfamiliar situations, orientation/place-finding problems and the experience of sensory overload
Dyscalculia, a difficulty to understand simple number concepts and to master basic numeracy skills; this includes learning number facts and procedures, telling the time, time keeping, understanding quantity, prices and money
Dysgraphia, a difficulty with writing. In addition to writing words that are difficult to read, people with dysgraphia tend to use the wrong word for what they’re trying to communicate
There are a number of explanations relating to what dyslexia is and why there is a difference in the way people with dyslexia and non-dyslexics think. Unfortunately, as I said earlier I am not scientifically minded, but the following seems to be the best and most popular explanation that I have found from multiple sources.
Right Brain vs Left Brain
The right side of the brain is where large scale/’big picture’ or global features of objects are processed. Information in relation to creating connections, linking information together, seeing relations and getting the ‘gist’ of things is also processed here. The dyslexic brain sees the essence of things: spotting the larger context, having abilities to see new, unusual or distant connections, to recombine things in a novel ways and see general inventiveness and best fits. However, the trade-off is people with dyslexia use the right brain more extensively than the left side, hence their difficulty with fine detail processing, which creates a difficulty with reading. Think of looking at a word, seeing the first letter and the last, then making up what’s in the middle, but still getting it wrong! Or think about looking at a forest, but finding difficulty in processing the individual trees.
The non-dyslexic brain in contrast however, is excellent at functions like precision, accuracy, efficiency, speed, automatic, reliability, replicability and focus, due to being able to use the left side of the brain more extensively.
The simplest explanation is the non-dyslexic brain excels at spotting differences, whilst the dyslexic brain excels at recognising similarities.
Advantages explained
Unfortunately, it is human nature to concentrate on just the disadvantages, but dyslexia confers many advantages within the police service, and is why I believe policing is such an attractive career option for dyslexics. These areas are linked to a range of skills, such as: ‘big picture’ thinking, problem-solving and lateral thinking abilities, an instinctive understanding of how things work, originality, creativity and exceptional visual-spatial ability. Many with dyslexia show the ability to think in 3D perspectives and to think in pictures. This has a potential trade-off of struggling with 2D perspectives such as images and writing on paper, and mirroring when writing, e.g. using the letter b instead of d, the number 6 instead of 9, and so on.
Many with dyslexia will show an ability to perceive more distant or unusual connections or to detect context and gist. The trade-off for this ability is a tendency to complicate certain simple tasks, and over-sensitivity to environmental factors such as noises, movements and other sensations.
Many dyslexics excel in the ability to perceive information as mental scenes that they construct from past personal experience, and many have the ability to reconstruct past events that they didn’t witness or to predict future scenarios. As you can see these are ideal strengths to put to use in policing scenarios, and many people will have instinctively used them without knowing.
Many individuals who have dyslexia can also show a certain set of specifically related artistic and entrepreneurial skills. Famous individuals with dyslexia and other learning difference dyslexia include, as previously mentioned: Albert Einstein, Bill Gates, Richard Branson, Sir Alan Sugar, Steve Jobs, Donald Trump, Winston Churchill, JFK, Agatha Christie, James Dyson, Leonardo da Vinci, Mother Teresa, Napoleon, Thomas Edison, Muhammed Ali, Tom Cruise, Cher, Orlando Bloom, Tommy Hilfiger, Andy Warhol, Beethoven, Mozart, John Lennon, Noel Gallagher, George Washington, Walt Disney, Picasso, Steven Spielberg, Will Smith, Whoopi Goldberg, Robbie Williams, Jamie Oliver, Daniel Radcliffe and Prince Harry – to name just a few.
I hope this article has helped someone in some small way to describe the complexities of dyslexia, and to understand that having a brain that thinks differently is a positive. ∎